

















 112 / 172
112 / 172

Abstracts of the 22
nd
National Congress of Digestive Diseases / Digestive and Liver Disease 48S2 (2016) e67–e231
e173
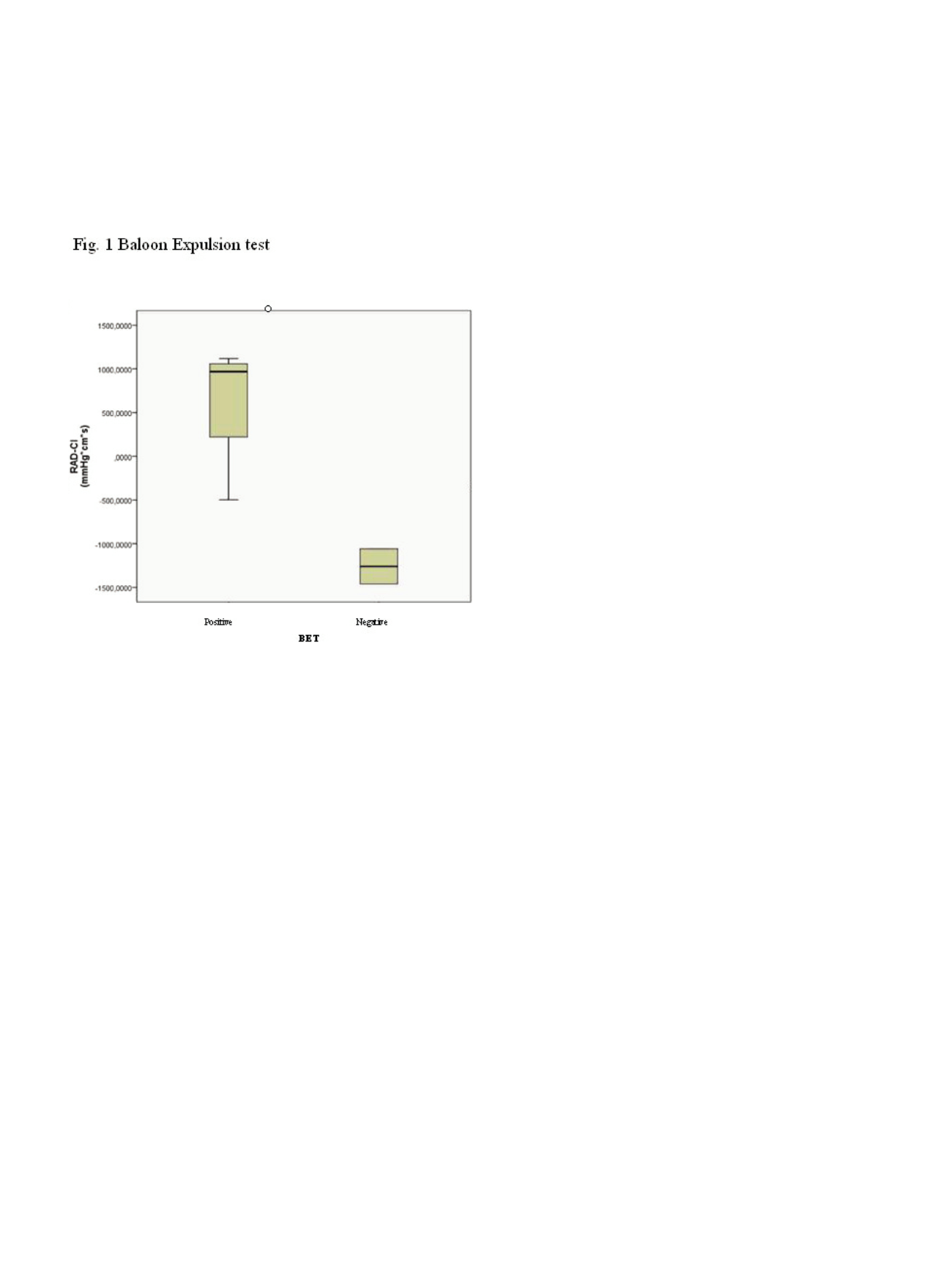
Results:
Correlation between 3D-HRAM and WPM was found
regarding maximum pressure (r=0.53, p<0.05), squeezing pressure
(r=0.85, p<0.001), RAIR (r=0.76, p<0.001), constant sensation (r=0.55,
p<0.05) and maximum tolerated volume (r= 0.63, p=0.005). Eighteen
patients showed a dyssynergic pattern at 3D-HRAM (9 type I, 9 type
II). RAD-CI was inversely related to BET (p<0.05) (fig.1) and this
correlation is stronger than that detected by using the traditional
RectoAnal Pressure Gradient (RAPG) (ns, p=0.17).
Conclusions:
Also in the evaluation of dyssynergic defecation
3D-HRAM shows a substantial agreement with WPM. This study
shows that RAD-CI show a correlation with BET better than RAPG.
RAD-CI could be an important index for the evaluation of dyssynergic
defecation.
P.09.5
DIVERTICULAR DISEASE: ALTERED RESPONSE TO ENTERIC
NEUROTRANSMITTERS IN HUMAN COLONIC LONGITUDINAL AND
CIRCULAR SMOOTH MUSCLE
Pallotta L.*
2
, Scirocco A.
2
, Ignazzi A.
1
, Maselli M.A.
1
, Cicenia A.
2
,
Carabotti M.
2
, De Toma G.
2
, Tellan G.
2
, Pezzolla F.
1
, Corazziari E.
2
,
Severi C.
2
1
Farmacologia Sperimentale Istituto di Gastroenterologia S. De Bellis,
Castellana Grotte (BA), Italy,
2
Università “Sapienza”, Roma, Italy
Background and aim:
Colonic diverticulosis (CD) represents an
asymptomatic condition that may predispose to the development of
uncomplicated and complicated diverticular disease (CDD). Several
alterations in muscle structure and enteric neural derangement
have been reported in both conditions, predisposing to colonic
dysmotility. Aim of this study was to investigate the presence of
functional and molecular alterations in human colonic muscle in CD
and CDD.
Material and methods:
Longitudinal and circular smooth muscle
cells (SMC) and strips were isolated separately from surgical
colon specimen of 9 patients (58<age<80years) affected either by
sigmoid CD or CDD and 9 patients (61<age<80years) submitted
to surgery for colon cancer. Contraction was tested in response to
acetylcholine (Ach1μM) or carbachol (CCh 1μM), whilst relaxation
to vasoactive intestinal peptide (VIP1μM). qPCR analysis was
performed for transcription of muscarinic M3, VIP-related receptors
(VPAC1,VPAC2,NPR-C) and eNOS. qPCR data were normalized to
b
-actin mRNA. Data are expressed as mean±SE, p<0.05 considered
significant.
Results:
In CD, longitudinal muscle showed a significant decrease
in Ach-induced contraction compared to control (cells: 9.8%±1.4 vs
16.8%±1.8, strips: 830±54 vs 1664±173 mN/cm2 respectively) and in
transcripts for M3 receptors (6.8±0.18 vs 7.98±0.45). CD longitudinal
muscle did not differ from control in terms of resting cell length,
VIP-induced-relaxation and transcripts for VIP receptors and
associated signals. In turn, CD circular muscle presented an impaired
relaxation in comparison to control (cells: 33.3%±8.3 vs 93.2%±1.4,
strips: 458±55 vs 1435±242 mN/cm2) associated to a significant
decrease of transcripts for VIP-related receptors and signals: VPAC1
(8.7±4.4 vs 15.6±0.1), VPAC2 (9.0±0.4 vs 13.2±1.0), NPRC (9.5±0.03 vs
15.2±0.3) and eNOS (10.3±0.9 vs 14.7±0.2). CD circular muscle did
not differ from control in terms of contraction. In CDD, besides the
impairment of relaxation, an inhibition of contractile response was
observed compared to control (6.5%±1.1 vs 17.7%±0.7).
Conclusions:
In CD and CDD colonic muscle presented an altered
response to enteric neurotransmitters associated to different
expression of their membrane receptors. These myogenic alterations
represent a further element contributing to colonic dismotility in
both conditions.
P.09.6
LONG TERM FOLLOW-UP OF RECURRENT/RESIDUAL COLORECTAL
ADENOMAS AFTER ENDOSCOPIC SUBMUCOSAL DISSECTION: A
SINGLE CENTER EXPERIENCE
Fiori G.*, Genco C., Ravizza D., Bravi I., De Roberto G., Trovato C.,
Crosta C.
Division of Endoscopy, European Institute of Oncology, Milano, Italy
Background and aim:
Endoscopic removal of recurrent/residual
colorectal polyps (RCP) is a challenging procedure due to low
effectiveness in radical resection, technical difficulties and high
rates of complications. Some retrospective studies described the
performance of endoscopic submucosal dissection (ESD) in this
setting, however few data are available on long term outcomes. Aim
of this study was to report our data on endoscopic follow-up in this
group of patients.
Material and methods:
We retrospectively evaluated a group of
consecutive patients who underwent ESD from 2011 to 2013 for
recurrent/residual colorectal polyps after one or more previous
treatments. Data regarding size and site of adenomas, endoscopic
technique, complications, histopathological examination and
outcomes of the procedure (complications, radicalness of resection,
rate of recurrence and need for re-retreatment) were evaluated.
Data are showed as mean±standard deviation or median with ranges
for discrete variables and percentages for continuous ones.
Results:
Thirteen patients (mean age 64.4±9.8 years, males 38.4%)
were included in the study. Median size of polyps was 20 mm (range
10-50 mm). Three perforations occurred during the endoscopic
procedures (23.1%) but were managed conservatively with clips
application. En-bloc resection was achieved in 7 patients (53.8%).
Histopathologic examination revealed low-grade dysplasia in five
cases (38.4%), high-grade dysplasia in seven cases (53.8%) and one
case of adenocarcinoma (7.7%). R0 resection was achieved for deep
margins in four cases (30.7%) and for lateral margins in 9 cases
(69.2%). In one case (7.7%) margins were not evaluable (Rx) because of
coagulation artifacts. The patient diagnosed with a malignant polyp
underwent surgical treatment for R1 resection evidence. At first
endoscopic control in two patients (16.6%) relapse of adenomatous
tissue on the post-ESD scar was observed during follow-up, which
was successfully removed endoscopically (in one with two sessions