

















 127 / 172
127 / 172

e188
Abstracts of the 22
nd
National Congress of Digestive Diseases / Digestive and Liver Disease 48S2 (2016) e67–e231
resting metabolism (REE; indirect calorimetry, Sensor Medics),
body composition (BIA Akern), food intakes/eating disorders (kcal/
macronutrients; 24 hr recall history), nutritional blood exams were
registered and recorded. Each patient followed a personalized
program: -medical checks, nutritional counseling, meal planning and
assistance at meals by an expert dietician; -individual psychiatric/
psychological sessions (to identify and treat core personality traits/
disorders in relation to obesity); - physical exercise planning. Results
were divided per sex.
Results:
Results on weight loss at 3, 6 and 9 months: see table.
Most patients lost a lot of weight; 7 obtained a mean loss of >20%
initial weight at 9months, but the programme is still in progress. 2
diabetics significantly reduced insulin therapy; one suspended the
treatment. All improved eating behaviour, reduced glucides/lipid
intakes. A better psychological well being was achieved also due to
peer group support and more physical exercise.
Conclusions:
Our experience on a difficult population of morbid
obeses, with a combined intensive nutritional rehabilitation
program was successful in terms of weight loss, eating behaviour
and subjective well being. With a patient targeted approach
(personalized dietetic and psychological therapy together with
the peer group support) patients developed a better insight on the
mechanisms underlining the development and maintenance of
morbid obesity
P.12.10
SMALL INTESTINAL BACTERIAL OVERGROWTH IS LINKED TO
VASCULAR DISEASE VIA VITAMIN K2-DEPENDENT MECHANISMS
Ponzani F.R.*
1
, Flore R.
2
, Scaldaferri F.
1
, Gaetani E.
1
, Gasbarrini A.
1
1
Internal Medicine and Gastroenterology, A Gemelli Hospital, Rome,
Italy,
2
Angiology, A Gemelli Hospital, Rome, Italy
Background and aim:
Matrix Gla-protein (MGP) is a vitamin
K2 carboxylation-dependent enzyme with inhibitory activity on
vascular calcification. MGP inactive form (undercarboxylated MGP,
ucMGP) has been recognized as a marker of cardiovascular disease
and is associated with increased arterial stiffness.
In Western populations, vitamin K2 request is mainly supplied by
gut bacteria since dietary intake is minimal. To investigate if ucMGP
levels may be reduced in patients with SIBO and if this could be
associated withincreased arterial stiffness/presence of vascular
calcifications.
Material and methods:
Consecutive patients with very low/low
Framingham risk score evaluated for gastrointestinal symptoms
suggestive for SIBO underwent abdominal aorta and peripheral
arteries doppler ultrasound to assess arterial stiffness (carotid
artery distensibility (mm)/pulse wave velocity, PWV (cm/sec)) and
the presence of vascular calcifications; vitamin K2 daily intake was
investigated by a nutritional questionnaire and a blood sample was
performed to quantify circulating levels of ucMGP. Patients with
conditions potentially affecting ucMGP levels were excluded (e.g.
diabetes mellitus, renal insufficiency). A glucose breath test was
used to confirm the diagnosis of SIBO. Statistics was performed
using r statistics package v. 3.1.2; data are expressed as median
(range) and frequency (%).
Results:
Thirty-nine patients were included in the analysis; median
age was 57 (41-50) years, 14 (35.9%) male, median K2 intake 29.6 (8-
103) mcg/day. SIBO diagnosis was confirmed in 12 (30.8%) patients.
As expected, circulating ucMGP levels were increased in patients
with vascular calcifications (6.7 vs 4.6 ng/ml) and indirectly
correlated with arterial distensibility (Spearman’s rho -0.596
p=0.05) and directly with PWV (0.535 p=0.0004).
Although vitamin K2 daily intake was lower in patients with SIBO
(18.9 vs 32.5 mcg/day p=0.05), as expected circulating ucMGP levels
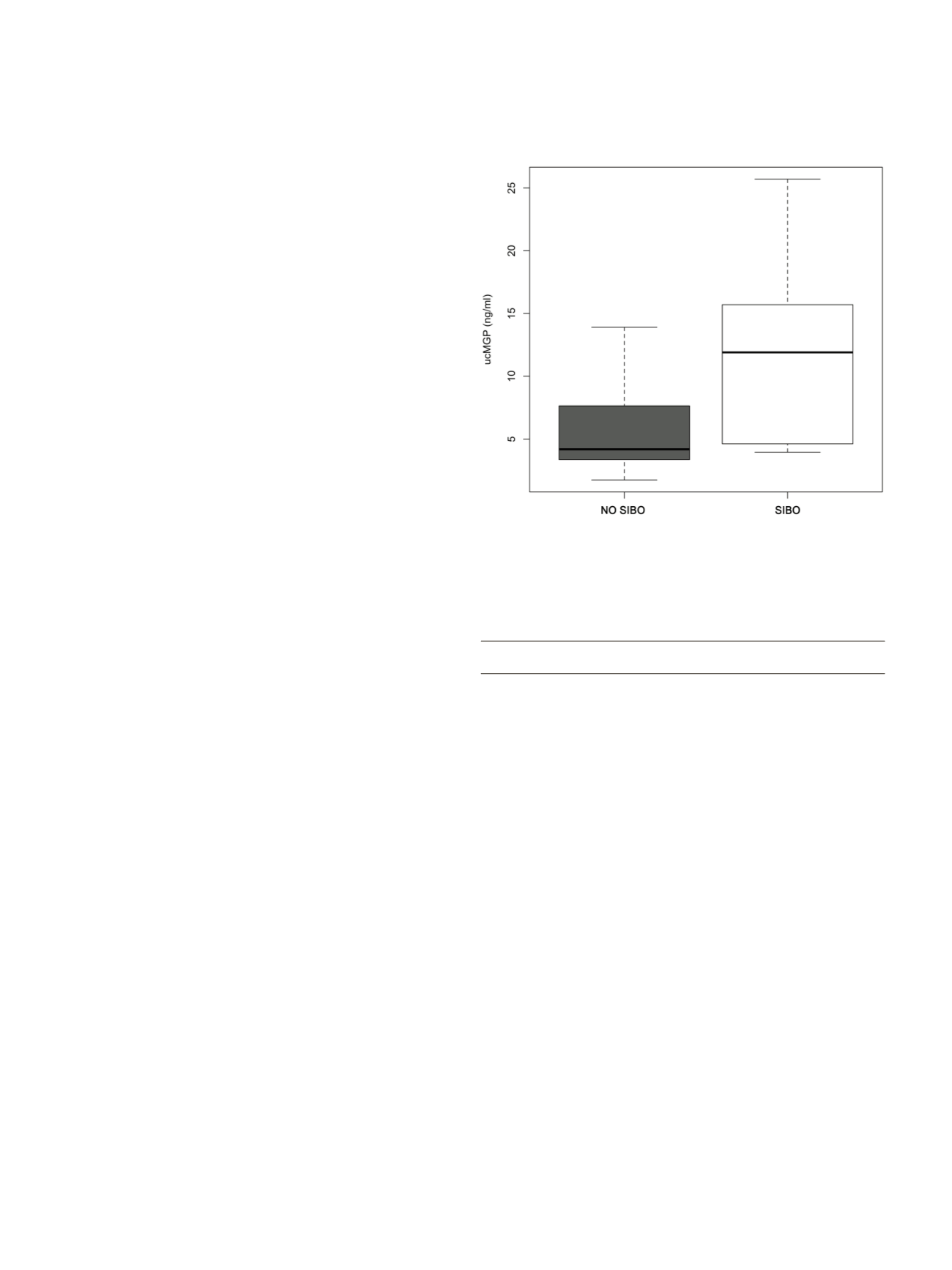
were independend of it (p=0.725). ucMGP levels were higher in
patients with SIBO (11.9 vs 4.2 ng/ml, p=0.003 Figure 1), who
presented vascular calcifications in 66.7% of cases (vs 51.8%) and an
increased arterial stiffness (distensibility 210 vs 255 mm, PWV 9.8 vs
8.2 cm/sec Figure 2).
Conclusions:
Dysbiosis may contribute to increase the risk of
vascular calcifications and increased arterial stiffness in patients
with SIBO, by increasing circulating levels of ucMGP due to reduced
vitamin K availability.
P.13 Colon 2
P.13.1
SPLIT-DOSING REGIMEN FOR BOWEL PREPARATION BEFORE
COLONOSCOPY: LOW-VOLUME PEG (POLYETHYLENE GLYCOL)
SOLUTIONS VERSUS LARGE-VOLUME PEG SOLUTION IN CLINICAL
PRACTICE
Saettone S.*, Reale E., Armellini E., Ballarè M., Crinò S., Montino F.,
Orsello M., Tari R., Occhipinti P.
Gastroenterology Unit, “Maggiore della Carità” University Hospital,
Novara, Italy
Background and aim:
Colonoscopy is the current gold standard
for the diagnosis and treatment of large-bowel pathologies and
for colorectal cancer screening. High quality colonoscopy is largely
dependent on the quality of bowel preparation, that has a large
impact on adenoma detection rate (ADR), caecal intubation rate
(CIR). Split dosing of large volume preparations seems to improve
efficacy of bowel preparation, improve ADR and patients acceptance
but there is no clear evidence in literature about split dosing applied
to low-volume formulations. Primary endopoint was to assess
efficacy of split-dose low-volume PEG solutions (PEG+BIS or PEG-
ASC) versus split-dose large-volume bowel preparation (PEG-ELS) in
unselected outpatients population; secondary endopoints were to
assess the acceptance, compliance, tolerability, safety profile.
Material and methods:
We retrospectively analyzed data from our
patients’ registry. Procedures from 5/12/2014 to 1/04/2015 have been
considered, including 427 patients using split-dose preparation.
Evaluation of efficacy was performed by using the Ottawa Bowel
Preparation Scale.