

















 129 / 172
129 / 172

e190
Abstracts of the 22
nd
National Congress of Digestive Diseases / Digestive and Liver Disease 48S2 (2016) e67–e231
Material and methods:
Twelve IBS patients, diagnosed ccording
to Rome III criteria (11F; mean age 44.2±15.5 yrs.: 2 constipation-
predominant, 3 dirarrhea-predominant and 7 with mixed IBS) were
treated with a low FODMAP diet, adequate in macro/micronutrients,
for 8 weeks. When entering the study (T0) and after 8 weeks (T2)
several assessments were carried out. These were an IBS-SSS
questionnaire referring to IBS symptom severity, a questionnaire
evaluating bowel habits using a scale from 0 (no symptom) to 4
(symptom present ≥75%), SF36 for quality of life, HADS for anxiety
and depression, Pittsburgh questionnaire for sleep disorders and a
bioelectrical impedance analysis to assess body composition.
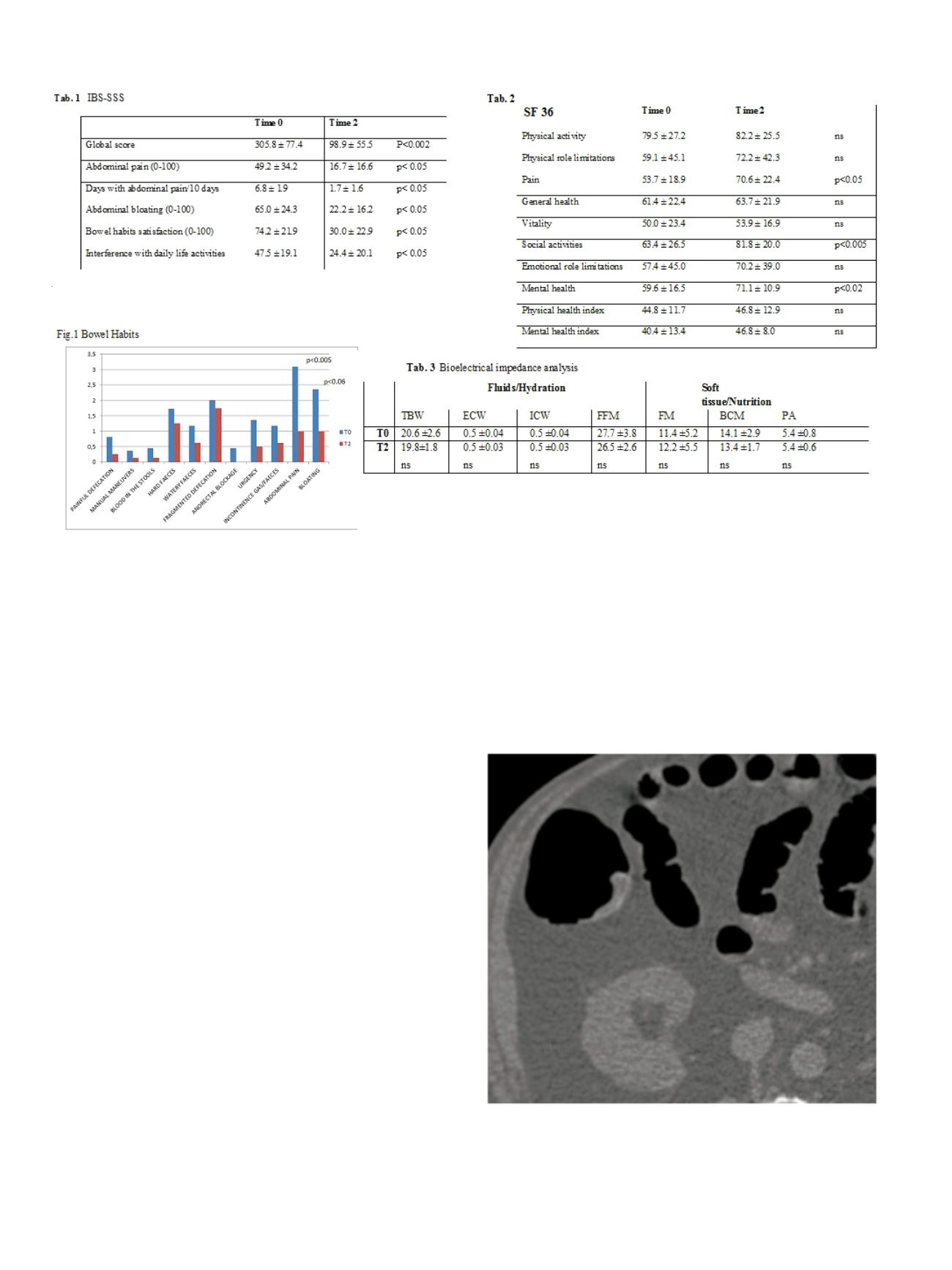
Results:
At T2 IBS-SSS improved (global score: 305.8 ± 77.4 vs 98.9 ±
55.5; p<0.002) (tab.1) together with bowel habits (fig.1) and quality
of life (tab.2). No change in sleep quality (6.0 ± 4.8 vs 5.0 ± 2.1),
anxiety (6.5 ± 3.6 vs 6.0 ± 3.5) and depression (5.6 ± 4.3 vs 6.6 ± 4.6),
BMI (23.6 ± 4.2 vs. 23.6 ± 4.5), body composition and extracellular
body water (Table 3) was noticed. The degree of relief using a scale
from 0 (total relief) to 7 (no relief) was 1.2 ± 1.0.
Conclusions:
The low FODMAP diet greatly improved IBS symptoms
as well as quality of life in IBS patients, without affecting BMI, body
composition and extracellular body water. Patients were highly
satisfied with their clinical improvement.
P.13.5
COLONIC FLAT LESIONS DETECTION USING 64-MDCT
COLONOGRAPHY, AND A COMPUTER AIDED DETECTION (CAD)
SYSTEM. RADIOLOGICAL-ENDOSCOPICAL CORRELATION
Efrati C.*
1
, Iafrate F.
2
, Cannaviello C.
1
, Finizio R.
1
, Piazza O Sed N.
3
1
ospedale israelitico, rome, Italy,
2
Policlinico Umberto I, Roma, Italy,
3
Ospedale Maggiore Policlinico, Milano, Italy
Background and aim:
To evaluate the ability of computer aided
detection (CAD) software to detect morphologically flat “non
polypoid” lesions at CT colonography. To correlate CT colonography
Examination with Endoscopy.
To create a hit list of top ten difficult lesion with Radiological and
Endoscopical correlation
Material and methods:
The CTC datasets of a total of 61 patients
with 74 endoscopically proven flat lesions were loaded onto a
workstation with CTC viewing software and reviewed with and
without CAD system by two radiologists experienced in CTC
interpretation, fully unaware of the colonoscopic report.
A total of 61 patients underwent fecal tagging preparation before
CTC. Mean reading time with and without CAD, sensitivity and
number of false positive were evaluated. Colonic localization as well
as histology of all lesions was provided.
Finally an expert reader put flat lesions under magnifying glass
creating a top ten list of most difficult lesions discovered on CT
Colonography with endoscopical correlation.
Results:
21 of 74 lesions were missed by reading CTC examination
without CAD. CAD alone detected 58 of 74 flat lesions. Two radiologist
in consensus using CAD software detected 62 of 74 lesions and two
lesions detected by CAD was not reported as flat lesions due to low
conspicuity. 39 lesions were of 3 mm in height, and 18 ranging in