

















 91 / 172
91 / 172

e152
Abstracts of the 22
nd
National Congress of Digestive Diseases / Digestive and Liver Disease 48S2 (2016) e67–e231
Results:
Exploratory laparotomy revealed a 4 cm stenotic lesion
in the cecum-ascending colon, with numerous peritoneal micro
nodules and adjacent lymphadenopathies. A carcinologic right hemi
colectomy was performed. Examination of the resected specimen
revealed a stenotic ulcerated lesion in the colonic wall in proximity
to the ileocecal valve and microscopic examination showed multiple
noncaseous granulomas composed of a central core of epithelioid
cells and multinucleated giant cells surrounded by a lymphocyte
cuff. In absence of acid-fast bacilli or foreign bodies at Ziehl–Neelsen
staining, a diagnosis of sarcoidosis was made.
Conclusions:
Only histologic examination of the surgical specimen
can yield a diagnosis of gastrointestinal sarcoidosis due to the non-
specificity of endoscopic and radiologic findings.
P.05.12
DIFFUSE INTESTINAL NODULAR LYMPHOID HYPERPLASIA (DNLH)
IN A PATIENT WITH EPIGASTRIC PAIN: A CASE REPORT
Capoferro E.*
1
, Ntakirutimana E.
2
, Dal Fior D.
3
, Colombari R.
3
,
Inturri P.
2
, Cristofori C.
2
, Rostello A.
2
, Checchin D.
2
, Bulighin G.
2
1
UOC Gastroenterologia B - Azienda Ospedaliera Universitaria
Integrata, Verona Borgo Roma, Italy,
2
UOC di Gastroenterologia
ULSS20, Verona San Bonifacio, Italy,
3
UOC di Istologia e Anatomia
Patologica ULSS20, Verona San Bonifacio, Italy
Background and aim:
Diffuse intestinal nodular lymphoid
hyperplasia (DNHL) is a rare disease involving either the entire small
intestine or the large intestine or both, characterized by the presence
of multiple small nodules, normally between 2 and 10 mm in
diameter. DNLH has been observed more frequently in children and
more rarely in adults in whom it is often associated with common
variable immunodeficiency (CVID) [1]. Symptoms include epigastric
pain, chronic diarrhea and intestinal obstruction. Pathogenesis is
often unclear.
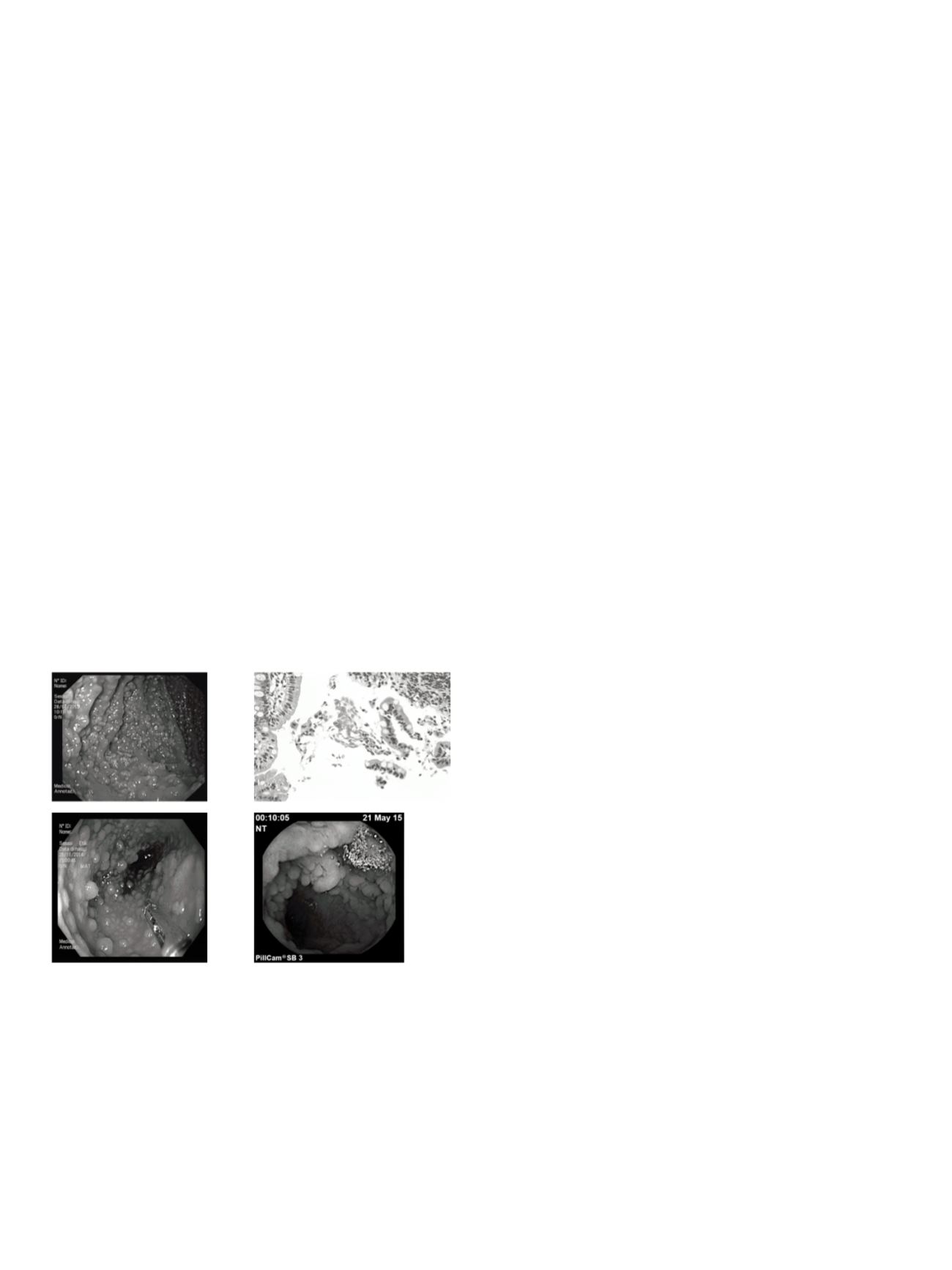
Material and methods:
We report the case of a patient with DNHL
in whom Giardia Lamblia and Helicobacter pylori eradication
relieved symptoms. In October 2014 a 44 - year- old woman was
admitted to our clinic for epigastric pain and diarrhea present
since June. Gastroscopy (EGDS) revealed inflammation of the
gastric antrum mucosa and multiple millimetric polypoid lesions
in the duodenum. Histological findings showed Helicobacter Pylori
gastritis and lymphoid follicular hyperplasia in the duodenum with
Giardia infection. The patient’s biochemical, serologic and stool tests
were normal except for serum Ig A reduction [2]. CVID was therefore
suspected. Ileo-colonscopy and video endoscopic capsule also
revealed multiple polypoid lesions. HP was eradicated and Giardia
was treated with metronidazole. The patient was referred to an
immunologist for complete investigation.
Results:
Both treatments completely relieved symptoms. The
endoscopic picture at 6 and 12 months was unchanged and histology
showed post treatment Hp and Giardia Lamblia eradication.
Conclusions:
Despite improvement of symptoms following
treatment, endoscopic and histological findings of DNHL persist in
time.
References:
1. Andreia Albuquerque. Nodula lymphoid hyperplasia in the gastrointestinal tract
in adult patients: A review.. World J Gastrointest Endosc 2014; 6(11): 534-540.
2. Postgate A, Despott E, Talbot J et al. An unusual cause of diarrhea: diffuse intesti-
nal nodular lymphoid hyperplasia in association with selective immunoglobulin
A deficiency (with video). Gastrointestinal Endosc 2009; 70: 168-169.
P.05.13
PANCREATIC MUCINOUS CYSTIC ADENOCARCINOMA METASTASIS
TO THE RECTUM
Carrara S.*, Brambilla T., Zerbi A., Repici A.
Humanitas Research Hospital, Rozzano, Italy
Background and aim:
Most patients with pancreatic cancer have a
metastatic disease at the moment of diagnosis. Usually pancreatic
cancer spreads to the liver, lymph nodes, and lung.
Material and methods:
A 38 years old woman presented with a
pancreatic mass and a rectal cancer. She was admitted to another
hospital because of abdominal pain. A colonoscopy revealed a rectal
adenocarcinoma. At CT a mass was observed in the pancreatic tail.
The patient was addressed to our Hospital for a multidisciplinary
approach. An endoscopic ultrasound (EUS) showed a malignant
mucinous cystic neoplasm of the pancreatic tail with infiltration
of the surrounding pancreatic parenchyma. An EUS-FNA confirmed
mucinous material.
Results:
A rectal EUS showed an ulcerative lesion, with convergence
of mucosal folds, corresponding to a thickened rectal wall with
loss of the layers structure that was strictly adhering to a nodule
in the mesorectum. It looked more like something coming from
outside the rectal wall, than a primitive rectal cancer, so that other
biopsies were obtained. The histological examination reported an
adenocarcinoma. The immunohistochemical (IHC) staining was
positive for cytokeratin 7, cytokeratin 20, and mildly positive for
CDX2. The final diagnosis was a rectal metastasis from pancreatic
cancer. A 18F-FDG-PET confirmed the hyperaccumulation in
the pancreatic tail and rectum. The patient received systemic
chemotherapy. At restaging, the rectal EUS showed a response, with
initial reconstruction of the layers. She underwent a distal pancreatic
resection. The pathological examination reported a mucinous cystic
adenocarcinoma (CK7+, CK20+, CDX2-/+), pT3N1R0.
Conclusions:
Pancreatic cancer metastasis to the rectum is very
rare. EUS can be helpful to differentiate a primitive rectal cancer
from an infiltration from the mesorectum. IHC staining for CK7 and
CK20 can help in diagnosing metastasis from pancreatic cancer.
P.05.14
MUCOSAL TEARS OCCURRED DURING COLONOSCOPY IN
OUTPATIENT WITH ULCERATIVE COLITIS: A CASE REPORT
Labianca O.*, Zulli C., Maurano A.
AOIU San Giovanni di Dio e Ruggi d’Aragona - Gaetano Fucito
Hospital - Digestive Endoscopy Unit, Mercato San Severino (Salerno),
Italy
Background and aim:
The term of Mucosal Tears (MT) is used
by several authors to describe linear mucosal defects and sharp
longitudinal ulcers, as a characteristic colonoscopic findings in
patients with collagenous colitis. We report a rare case of MT