

















 86 / 172
86 / 172

Abstracts of the 22
nd
National Congress of Digestive Diseases / Digestive and Liver Disease 48S2 (2016) e67–e231
e147
percentage perforate the bowel, leading to acute abdomen and
requiring surgical intervention. Foreign bodies such as dentures,
fish bones, chicken bones, toothpicks and cocktail sticks have been
known to cause bowel perforation
Impaction, perforation, or obstruction often occurs at GI angulations
or narrowing. Hence, patients with previous GI tract surgery or
congenital gut malformations are at increased risk
Material and methods:
We report the case of a 75 years-old male
patient without previous surgery presented with intermittent
abdominal cramps and diarrhea of 2 months’ duration. Two months
earlier, he had also experienced hematochezia on three occasions.
On physical examination, bowel sounds were normal and there
was no abdominal organ enlargement, tenderness, or rebounding
pain. Digital rectal examination was unremarkable. Physical
examination showed a diffuse tenderness of abdomen without
defense. Clinical and biochemical data were negative. An x-ray of
the abdomen showed in hypogastrium a calcific body compatible
with bone fragment that was projected at the level of the sigmoid
colon. Excluded perforation we proceeded to recto-sigmoidoscopy
previous preparation with macrogol.
Results:
At 25 cm from the anal verge, the mucosa was edematous
and hyperemic and an impacted foreign body was present. We
proceeded to remove it using biopsy forceps, a silk tie was looped
around the impacted bone and then gently pulled caudally as it
exited the anus. No evidence of perforation or other complications
except presence of one pressure ulcer on the mucosal wall. After
removal of the bone, the patient became asymptomatic without any
residual symptom.
Conclusions:
It is therefore described a case in which poorly
suggestive symptoms and a non-specific examination has allowed
early detection and to target a targeted endoscopy with a rapid
resolution of symptoms. Our patient was not aware of the ingestion
of the foreign body.
Osseous esophageal foreign bodies are potentially dangerous as
the risk perforation always exist. Safe extraction or dislodgment
of an osseous foreign body can almost always be performed with
the endoscope stating an adequate preliminary evaluation and the
selection of proper equipment. After recognition of the impacted
foreign body, the patient was managed endoscopically with
resolution of symptoms.
P.05.2
FIRST CASE OF SMALL BOWEL ADENOCARCINOMA DETECTED
WITH THE NEW 360° PANORAMIC-VIEWING CAPSULE
ENDOSCOPY SYSTEM
Marino R.*
1
, Tontini G.
2
, Lumachi V.
1
, Gendarini A.
1
, Leoni P.
1
1
Gastroenterology and Digestive Endoscopy Unit, AO Lodi,
Gastroenterology and Digestive Endoscopy Unit, IRCCS Policlinico San
Donato, Milano, Italy,
2
Gastroenterology and Digestive Endoscopy,
IRCCS Policlinico San Donato, Milano, Italy
Background and aim:
Small bowel tumors (SBT) are rare, accounting
for only 1-3% of all gastrointestinal neoplasms [1]. Nonetheless,
among patients undergoing small bowel capsule endoscopy (SBCE),
neoplastic lesions can be detected in 2-9% of cases [2,3]..
Material and methods:
Here, we report the case of a 52 years
old outpatient presented for iron deficiency anaemia (Hb 7,4 g/dl,
ferritin 7 ng/ml), asthenia and dark discharge stools occurred after
oral intake of non-steroidal anti-inflammatory drugs without any
gastroprotection.
An immediate esophagogastroduodenoscopy showed antral ero
sive gastritis with no evidence of Helicobacter pylori infection
and subsequent ileo-colonoscopy was negative. Overt bleeding
stopped spontaneously and patient received medical treatments
based on proton pump inhibitors (esomeprazole 40 mg/24h) and
iron supplement. One month later, blood tests revealed persistent
iron deficiency anaemia (Hb 9 g/dl, MCV 72 fL, ferritin 10 ng/ml)
and positive fecal occult bleeding tests (3/3 samples). Therefore,
SBCE was performed using the newly introduced CapsoCam® SV1
(CapsoVision Inc, Saratoga, USA).
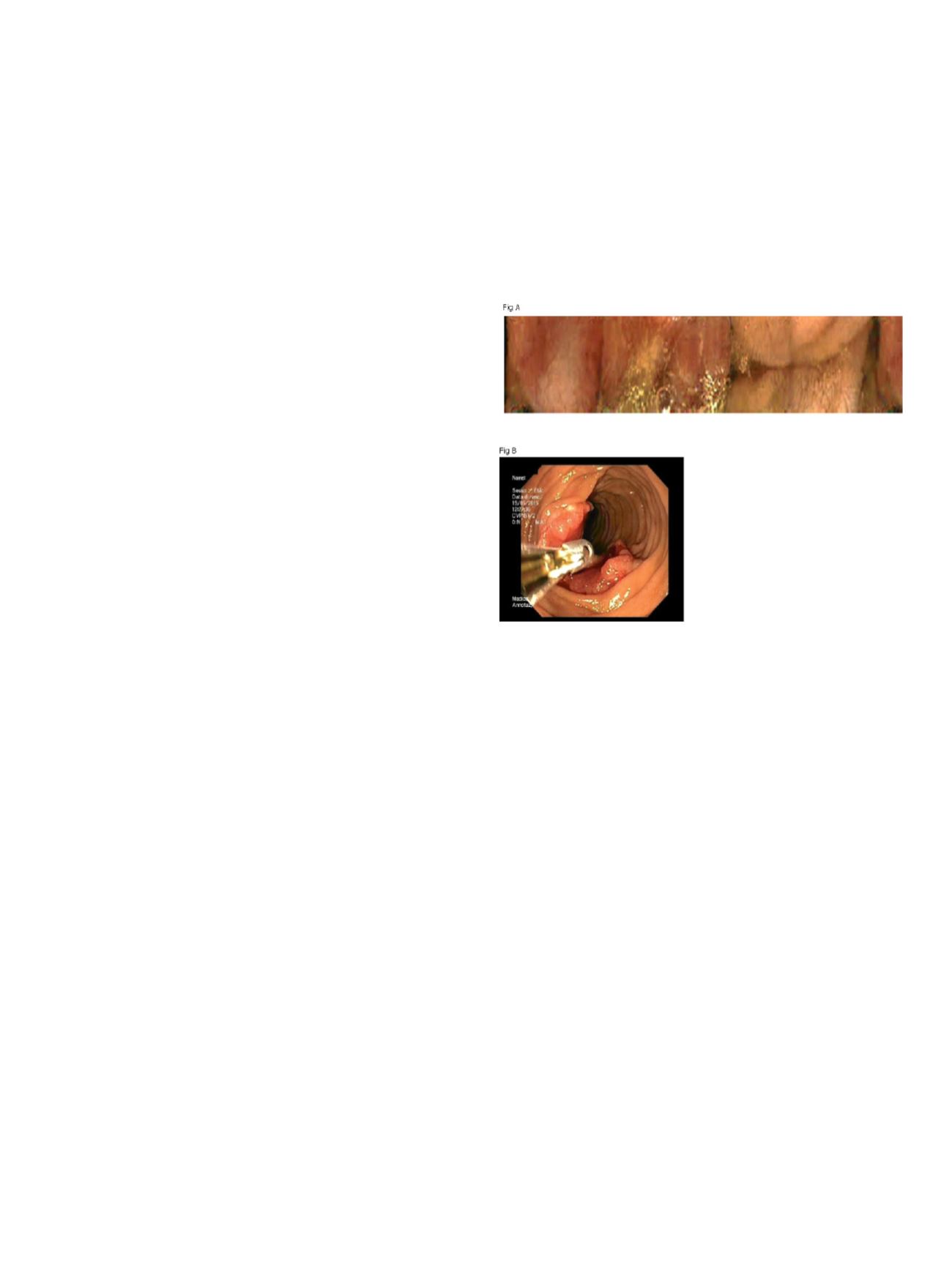
Results:
The SBCE explored the entire small bowel and the video
image quality always scored as optimal. The lateral view allowed a
clear visualization of an ulcerated nonbleeding lesion with central
depression in the proximal jejunum (fig A). The following
enteroscopic inspection confirmed the lesion site and the
macroscopic appearance (fig B). Histological analysis lead to the
diagnosis of adenocarcinoma and to surgical resection.
Conclusions:
The newly introduced CapsoCam® SV1 is a wire-free
device for SBCE with long lasting battery life, and 12-20 frames per
second captured by four lateral cameras to enable a 360° panoramic
view of the entire small bowel [4,5]. CapsoCam® SV1 has a detection
rate and a safety profile comparable to other SBCE with frontal view
in patients suffering from obscure gastro-intestinal bleeding or
with suspected Crohn disease [4-6]. This represents the first case of
jejunal adenocarcinoma discovered with Capsocam® SV1. Further
study should now evaluate the role of CapsoCam® SV1 as a new
standard in patients suspected for to have SBT.
References
1. Neugut A, et al. Cancer Epidemiol Biomarkers Prev 1999; 7:243-51
2. Cobrin GM, et al. Cancer 2006;107:22-27
3. Rondonotti E, et al. Endoscopy 2008; 40 (6): 488-495
4. Pioche M, et al. Endoscopy 2014 ; 46(6) : 479-84
5. Friedrich K, et al. J Gastroenterol Hepatol 2013 ; 28(9):1496-501
6. Tontini GE, et al. Accepted abstract UEG Week 2015
P.05.3
A RARE CASE OF GASTROINTESTINAL BLEEDING
Padula D.*, Lenti M.V., De Quarti A., Biagi F., Carnevale Maffe’ G.,
Alvisi C., Miceli E., Corazza G.R.
IRCCS Fondazione Policlinico San Matteo, Pavia, Italy
Background and aim:
A 48 old male was admitted to our clinic
for investigate a recurrent low gastrointestinal pain. In 2013 he
presented an episode of important lower gastrointestinal bleeding
causing severe anaemia which subsided spontaneously. In that
occasion a colonoscopy showed dilated tortuous sub-mucosal
veins through the entire explored tract (until the trasverse colon).
A contrast abdominal TC excluded vascular stenosis. Two sessile
polyps found in the sigma were excised in a second time, the
histology revealed a tubular adenoma with severe dysplasia. A